 Have you ever heard a runner say, “I have runners knee”? Patellofemoral pain syndrome (PFPS), also known as “runners knee” is the most commonly reported running injury and pain is located under the knee or on the inner side of the knee. It is likely related to poor mechanics such as increased hip adduction (thigh bone moving inward towards the center of the body) and hip internal rotation creating malalignment of the lower extremity joints (Noehren et al., 2010). Have you ever seen pictures of yourself, or your friends, running and it looks like the runner is knock-kneed or very little space between the knee of the leg that is in contact with the ground and the leg that is in swing? Hello weak hip abductors! Now it is true that some women have what is called a larger Q-angle (thank you, child-bearing hips!), so the way their thigh bone comes out of the pelvis will be more angled if you will. But you have read about weak hip abductors in my previous blog posts. Refresh your memory by reading the gluteus medius and piriformis blogs!
Iliotibial band syndrome (ITBS) accounts for 12% of all running related injuries (Strauss et al., 2011). ITBS is typically characterized as pain on the outer side of the knee. ITBS is quite interesting because most have accepted the theory that ITBS is a friction syndrome or a rubbing between the bottom portion of the iliotibial band and a bony projection on the end of the thigh bone next to the knee. This area of friction is referred to as the impingement zone. Other theories that cause ITBS exist that make sense and are supported in peer-reviewed scientific literature. For example, the iliotibial band is not a lone structure, but is connected to a thickened portion of the lateral fascia lata, a fibrous tissue that wraps around all the musculature composing the thigh (think sausage casing) and anchors into the femur (thigh bone) (Fairclough et al., 2007). At the other end of the iliotibial band, it is attached to the tensor fascia latae (TFL) muscle, which is guess what??? That’s right, another hip abductor and internal rotator! Okay, it aids in hip flexion too. In a study of 24 distance runners with ITBS, Fredericson and colleagues (2000) noted that all legs afflicted with ITBS had strength deficits in both the gluteus medius and the TFL and, more important to my readers, correcting the strength deficits lead to resolution of the problem. In a lecture by physical therapist Dr. Brent Brookbush, he said, “In my clinic, 9 out of 10 cases of ITBS are from a tight/overactive TFL muscle, not from an impingement at the site of pain". So, all those people that try to foam roll their iliotibial band really aren’t doing a darn thing, because the problem is up higher on the hip and should be foam rolling/applying pressure with a therapeutic device on the TFL. These types of strength deficits can be determined by chiropractors and physical therapists through manual muscle testing. Movement screenings that I offer my runners can also be predictive/prehab for the above issues. Just one of many reasons to hire Run With Gina in your quest for the best half/full marathon training and racing experience possible. Fight ON! Coach Gina Runner Image: Rosy Castro References: Fairclough, J., Hayashi, K., Toumi, H., Lyons, K., Bydder, G., Phillips, N.,…Benjamin, M. (2007). Is iliotibial band syndrome really a friction syndrome? Journal of Science and Medicine in Sport, 10, 74-76. Fredericson, M., Cookingham, C.C., Chaudhari, A.M., Dowdell, B. C., Oestreicher, N., & Sahrmann, S.A. (2000). Hip abduction weakness in distance runners with iliotibial band syndrome. Clinical Journal of Sports Medicine, 37(4-5), 437-439. Noehren, J., Scholz, J., & Davis, I. (2010). The effect of real-time gait retraining on hip kinematics, pain, and function in subjects with patellofemoral pain syndrome. British Journal of Sports Medicine, 45, 691-696. Strauss, E., Kim, S., Calcei, J., & Park, D. (2011). Iliotibial band syndrome: Evaluation and management. Journal of American Academy of Orthopaedic Surgeons 19, 728-736.
3 Comments
 Training for distance running events is a time-consuming endeavor and takes the right balance of work, family, and training to be able to achieve running goals or really any goal. Although any male or female can find the right combination of balance, it seems that this is still more of a challenge for working mothers. Back in 2010-11, I was training for the Boston Marathon; putting in more training than ever, for me. At the time, I ran with several females in a running group and many times I heard them say that they did not have time to train enough to achieve their goals due to family responsibilities. Not being in that situation at the time, I had no room to argue against it or make suggestions. When the 2011 Boston Marathon race day came along, I sat on the bus to the starting line next to a woman that told me that she was a school teacher, had three children under 9-years old, lives in upstate New York and had to train through a brutal winter that year, and due to her family responsibilities, she ran in the dark, in cold temperatures while her children were asleep. Ah ha! When there is a will, there is a way and this random woman modeled positive behaviors towards goal achievement. It is true that some people just want to run without goals and that is okay, but for those who desire to achieve goals and be the best runner they can be, this blog post is for you. Some of this may sound like common sense, but after working one-on-one with distance runners, I can say with certainty that many people see black and white in their life with no shades of grey. The magic can happen in the bleak grey areas, if you shed the light on those invaluable opportunities in your day.
In 2013, Archer and colleagues reviewed data from the American Heritage Time Use Study, which revealed a significant decline in physical activity and increase in sedentary behaviors of mothers between 1965-2010. It will come as no surprise that current sedentary behaviors are associated with screen time accessibility; social media, Apple T.V., Amazon Prime, Netflix…sound familiar anyone? It is true for men, women, and children. Also, a big change from 1965 to current times is the number of mothers in the workforce. Mailey and McAuley (2014) state, over 70% of mothers currently work and 50% of them were active prior to motherhood, yet are no longer active to amounts that benefit health. Working mothers suffer from “role overload” as still often the person responsible for domestic responsibilities on top of work responsibilities. Interestingly and paramount to the current blog post, research has determined that working mothers more than likely have the motivation to change physical activity behaviors, but are lacking in self-efficacy and self-regulatory strategies towards physical activity planning, adoption, and maintenance. Yes! My two favorites from my exercise and sports psychology classes: self-efficacy and self-regulation. This, folks, is where we shed light on the grey areas. Self-efficacy is described as perceived capability based on ability. If one believes he/she does not have the ability to fit training into his/her schedule, then it will be impossible. On a more positive note, self-efficacy (or one’s ability) can be fostered by past performance accomplishments, vicarious experiences, social persuasion, and physiological/affective states. Do you remember what it felt like when you were your fittest or fastest? This is the power of past performance accomplishments and the catalyst for physiological/affective states. When you see your friends on social media accomplishing their goals (say, qualifying for the Boston Marathon), can you literally feel their joy? This is the power of vicarious experiences. Do you see your friends enjoying running groups or getting faster with a personal coach and want the same for yourself? This is power of social persuasion. Self-regulation according to Bandura (1988) is setting goals and planning actions to achieve said goals. In a basic sense, this is problem solving. Problem solve all that stands in the way of you and your goals by identifying the barriers to your success. This is where I think mothers have issues. They know what the barriers are but only see black and white – “I can or cannot achieve that”, instead of “how can I achieve that?”. They think “I cannot because I must go to work, shuttle kids here and there, make dinner, do laundry, and on and on” and “I feel guilty for having ‘me’ time”. Like the woman on the bus in Boston, the only time she could run was when her children were sleeping, so that is what she did. Although not the most ideal option, some people run for 30 minutes during their lunch break and throw in another 30 minutes during their kids practice of whatever sort. Do you get stuck in traffic after work? Why not run while the traffic settles down? That extra 20-30 minutes sitting in traffic could have been 2-4 miles of running. Need to rush home to get the kids to practice? Thank goodness for carpool. Friends and family working towards each other’s goals together. Need to get dinner ready? Three cheers for the old crock pot or Sunday night meal prepping! Can’t get up off the couch because the magnetic pull is too strong? Don’t get on it to begin with. Just lace up your running shoes and hit the pavement first. I can almost guarantee that going for an easy training run will energize you before it will zap you of all that you have. The couch, on the other hand, will suck you in and you will become one with it and drain you of what you have left for the day. I must point out again, a lot of this is common sense, but you must ask yourself, “What stands in the way of me and common sense (the highway to my goals)?”. I was once in a class for coaches and trainers and the lecturer asked, “Who do you think is your biggest competition? The coach down the street? The gym across the street?” Nope, the answer was the couch. And if it is not the couch, it is the barstool at happy hour, the driver’s seat of your car in the slow lane during traffic hour, or maybe just giving more of yourself, not sharing responsibilities with other adults. Teamwork makes the dream work! Fight ON! Coach Gina Runner Images: Darryl, Tricia, and Ruby Sol. Danny and Melissa Magalei. Mark, Cristal, Winter, and Frankie Estrada References: Archer, E., Lavie, C. J., McDonald, S. M., Thomas, D. M., Hébert, J. R., Taverno-Ross, S. E.,…Blair, S. N., (2013). Maternal inactivity: 45-year trend in mothers’ use of time. Mayo Clinic Proceedings, 88(12), 1368-1377 Bandura, A. (1988). Self-regulation of motivation and action through goal systems. In V. Hamilton, G. H. Bower, & N. H. Frijida (Eds.), Cognitive perspectives on emotion and motivation (pp.37-62). Norwell, MA: Kluwer Mailey, E. L., & McAuley, E. (2014). Impact of a brief intervention on physical activity and social cognitive determinates among working mothers: A randomized trial. Journal of Behavioral Medicine, 37, 345-355.  Runners commonly have issues with piriformis syndrome, which is a literal pain in the butt, but it is difficult to determine the cause, so we are going to take a peek at functional anatomy and what research has supported in the treatment of piriformis syndrome.
As a very basic description, the piriformis muscle arises from the front portion of the sacrum (tailbone) and attaches to the femur (thigh bone) and its main function is hip external rotation (thigh bone rotating in an outward direction), aids in hip abduction (thigh away from the body), and aids in hip extension. Hip extension is what creates forward propulsion of the body during running. Due to my experiences with runners, I always think of the orientation and relationship of the pirifomis with the gluteal muscles. Dr. Shirley Sahrmann (2002) discusses the synergistic relationship of the piriformis with the gluteus maximus (GM) in hip extension. The GM is the main muscle of hip extension and the piriformis is one of the “helpers” in hip extension. Like all muscles, the piriformis may be subject to pain associated with muscle shortening from overuse as seen in synergistic dominance. Synergistic dominance is what occurs when a prime mover muscle is shut down and the helper muscle picks up all the work, making it too big for your britches, or just too tight and strong. Dr. Sahrmann does mention that the GM is a muscle that is frequently weak and the piriformis work load increases. Pain may also be from weakness of the muscle from lengthening. This pain is a literal pain in the butt and I unfortunately have had an issue with a weak, lengthened piriformis muscle, as diagnosed by a physical therapist (PT) a few years ago. I specifically remember the PT telling me, “Your marathon training is asking your gluteal muscles and pirifromis to do something they’re not strong enough to do.” I was reminded of this when Dr, Sahrmann said that it is a misconception that participating in a sport places adequate demands on musculature to elicit normal performance. In my case, I thought the dynamic nature of running would be enough strengthening of my running muscles to avoid weaknesses. This is a strong case for prehab exercises. I am all for prevention instead intervention, which is the point of many of my blog posts! Tonley and colleagues discuss piriformis syndrome in a 2010 case report of a subject complaining of “deep buttock pain”. The authors theorized that when the GM is weak, it accommodates abnormal movement patterns at the hip and consequently contributing to excessive lengthening of the pirifomis during functional activities. Muscle testing revealed weakness in the hip abductors, extensors, and external rotators. The subject participated in eight physical therapy sessions during a 3-month intervention. The intervention included exercises that were done at home in three, 4-week progressive exercises phases. Two weeks post intervention the subject declared no buttock pain and increased strength in the hip abductors, extensors, and external rotators. One year post intervention the subject still reported remaining pain free in the buttocks and had resumed sporting activities that were sidelined by pain. I think it is important to point out that synergistic dominance and muscle lengthening is often due to what we are doing when we aren’t running; sitting in the car, sitting at your work space, sitting on the couch, sitting in the bar, sitting with your legs crossed…sitting! Don’t ever forget movement is medicine and the one hour you may spend running, has nothing on all the hours of sitting throughout the day! By the way, if you want to know what the exercises in the pirifomis syndrome case study were, contact me at runwithgina@gmail.com Fight ON! Coach Gina Runner Image: Kay Kay Weir References: Sahrmann, S. A., (2002). Diagnosis and treatment of movement impairment syndromes. Philadelphia, PA: Mosby. Tonley, J. C., Yun, S. M., Kochevar, R. J., Dye, J. A., Farrokhi, S., & Powers, C. M. (2010). Treatment of an individual with piriformis syndrome focusing on hip muscle strengthening and movement reeducation: A case report. Journal of Orthopaedic & Sports Physical Therapy, 40(2), 103-111.  Twice last week I had runners comment to me about the mental aspect of long training runs and endurance races. This is something that many struggle with. It is true there are many factors that play into both the mental and physical “wall,” such as training status, hydration, nutritional practices, and pacing strategies. Regardless of the struggle and failure to meet time goals in a negative mental state, I often hear “but I didn’t give up, I kept going”. There is no doubt that endurance athletes are a special breed of humans. Research using validated psychological instruments has determined that marathon runners have innate, desirable personality profiles of less depression and anxiety and greater emotional stability and psychic vigor compared to non-runners (Raglin, 2001).
None the less, some still have mental demons that try to take them down. As runners, we just want to run, run, and run. However, for those of you that struggle with the demons or those that are ready to find out where there maximal potential as a distance runner is, you should incorporate mental training into your preparation. Mental training can help you prepare to combat the stinking thinking that comes with fatigue, boredom, pain, performance anxiety, and that little devil that takes a spot on your shoulder, negative self-talk. Thanks to some cognitive-behavioral strategies from the sports psychology world, we will be taking a glimpse at some psychological skills training techniques that you can incorporate into training to make you more mentally resilient. Imagery: Imagery is the most researched psychological skill for athletic performance enhancement. Vealy and Greenleaf (2010) discuss the power of imagery in performance enhancement with the simple definition of creating or re-creating a situation or experience in the mind. The most powerful aspect of said practice is how the brain processes virtual images as true stimulus. One way to practice imagery during mental training is to recall positive and negative times in a previous race situation. With the negative image, one practices visualizing overcoming fatigue at that point in the race, turning it into a positive experience for better race outcomes. We all have heard the saying, “seeing is believing”. If you see it in your head, you can help it come to fruition. Play out in your head how you want the race to go and how you want to feel in the moment. With positive images, recall the happiness, strength, and pride you felt and recreate it over and over in your head. Positive self-talk: Self-talk is deployed to reconstruct negative words into positive phrases. Turing self-talk such as “my legs are heavy and hurt” into phrases like “this is a challenge, but I am in it to win it in my head and I have prepared for this day” is an example of positive reconstruction. Positive reconstruction aids in refocusing on the task at hand, therefore augmenting control over running and being able to focus on performance cues, such as reminding yourself, “head up, shoulders relaxed, drive the knees forward, and push off the ground” (Barwood et al., 2008). Goal-setting: Goal-setting is so incredibly vital to marathon running performance and is worthy of its very own future blog post, so I will only give a brief description. Outcome goals are end goals, such as finishing time goals or age group placement goals. These goals, when matched with your level of ability, can help drive training so that you end up at the starting line feeling like a well-oiled machine, thus increasing confidence. Process goals are goals that you turn to throughout the race to help you get through it. An example would be planning when you will take in hydration and nutrition during the race to make sure that your engine remains optimally fueled. Another example is setting goals like “if I feel the need to walk, I will only walk the hydration stations”. A process goal can also be “my only goal is to not walk, because this could take several minutes off my previous marathon effort when I did walk”. Process goals are focusing on finishing the race by breaking it into phases. Some people can handle it my counting miles, whereas others cannot. You can also just count the “kills”, the number of people you pass on the race route that you had been hunting down as your process goal to pass more people than pass you. In a research experiment of psychological skills training, 18 male endurance runners ran for 90 minutes on a treadmill in a room set at 86 degrees Fahrenheit. The runners were blinded to the run pace and distance, but had control of slowing or speeding up the treadmill. Previous research on running in the heat has identified negative mental aspects such as; decreasing motivation, altering arousal, and creating negative mood states. Over the next four days, the runners were then given four, one hour sessions of psychological skills training, including mental imagery, positive self-talk, and goal-setting toward running in the heat. In a subsequent blinded 90 minute treadmill test with the ability to slow or speed the treadmill, the runners ran 8% longer in the same thermal conditions after psychological skills training (Barwood et al., 2008). If the mental aspect of training and racing is something you struggle with, you can find books on Amazon with the skills that I highlighted in this blog post. You must be realistic and know that if you haven’t trained or fueled properly for the distance or are training and racing through a true injury, psychological skills won’t pull you through to a personal best. Fight ON! Coach Gina Runner Image: Kimberly Grady References: Barwood, M. J., Thelwell, R. C., & Tipton, M. J. (2008). Psychological skills training improves exercise performance in the heat. Medicine & Science in Sports & Exercise, 40(2), 387-396. doi: 10.1249/mss.0b013e31815adf31. Raglin, J. S. (2001). Psychological factors in sport performance: The mental health model revisited. Sports Medicine, 31, 875-890. Vealy, R. S., & Greenleaf, C. A. (2010). Seeing is believing: Understanding and using imagery in sports. In J.M. Williams (Ed.), Applied sports psychology: Personal growth to peak performance (6th ed.) (pp. 267-299). New York, NY: McGraw-Hill. 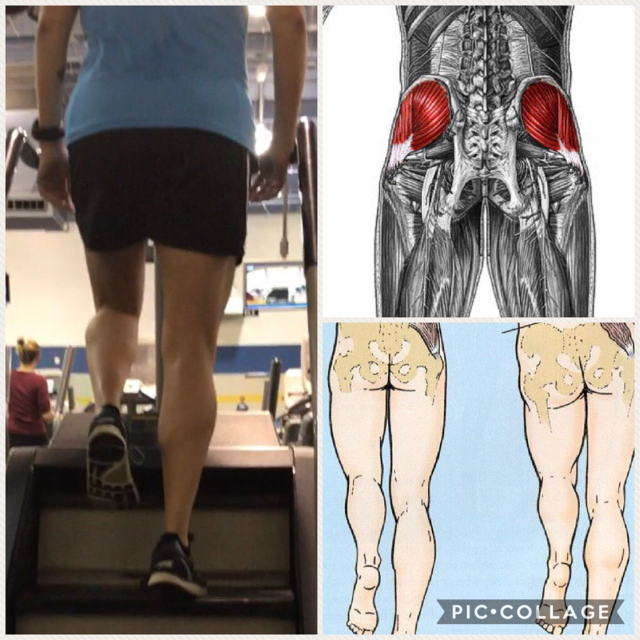 As stated in my previous blog post, “Cross-training can improve run performance”, I absolutely love the StairMaster Gauntlet machine, which is also called the Step Mill (if you didn’t read the post before this one, please do). I decided to expand on why that particular machine is useful for runners that are injured, injury prone, in the off-season, and really any gym goer that wants to move better in their activities of daily living, including just walking down the sidewalk.
In the pic collage above, the picture on the left is me on the StairMaster. Please ignore the scoliosis and slightly turned out stance foot. Haha! Just pointing it out if there are any observant critics out there. The illustration on the top right shows the anatomical location of the gluteus medius (glute med) muscle. The left half of the bottom right illustration demonstrates if the glute med is properly contracting, it will hold the hip opposite of the stance leg level. If it is weak, not contracting, or not “firing” properly, it will cause the opposite hip to drop as shown in the right half of the illustration. As observed in the picture of me, my left hip is being held pretty level with the hip of the stance leg or the leg that is still in contact with the revolving stairs. When we walk or run in the forward direction, we are doing so in the sagittal plane of motion. Glute med stabilizes the hips in the frontal plane of motion, so for simplicity reasons, think left to right or lateral to the body. Given that description, the primary function of glute med is to abduct the hip joint, which means to move lateral, away from the body. A side stepping motion, would be targeting the glut med. This motion, side stepping can be done on the StairMaster. Another reason why I love the machine! Because the glute med has anterior (front), middle, and posterior (rear) fibers it is a contributor to other motions at the hips as well, including hip flexion and extension. Some runners do a dynamic warm-up, mobility exercise, or neuromuscular control exercise called, walking high knees. Basically, walking high knees is an exaggerated hip flexion exercise, where you thrust your knee forward so that your thigh is parallel or just above parallel to the floor. This exercise can be done on the StairMaster. Because the stairs are moving it will provide a greater challenge to the core muscles to stabilize the single leg stance for more bang for your training buck! Additionally, one can do an exaggerated hip extension at toe off of the stance leg while on the StairMaster. I did say that the glut med “contributed” to hip flexion and extension, so there are other prime mover muscles also being targeted, but the point is that the StairMaster has a lot to offer runners and anyone that has weak hip musculature. The above may sound like jibber-jabber, but if I said the words iliotibial band syndrome (ITBS) or patellofemoral pain syndrome (PFSP), suddenly I may be speaking runners language. PFPS, also known as “runner’s knee” accounts for approximately 20% of running related injuries. PFPS occurs when the abductor musculature is weak, allowing for an increase in femoral adduction (thigh moving in) in the frontal plane (Dierks et al., 2008). This is the exact motions that glute med prevents when it is strong. Therefore, weak glute med can contribute to PFPS. Fairclough and colleagues (2007) suggest that ITBS is predominately a proximally based dysfunction of weak hip abductors, which decreases the control of thigh moving laterally. Glute med being one of the hip abductor muscles. When I screen my runners I often find weak gluteus medius muscles on most of them. This muscle is so vital to performance not just when running, but walking and moving in general. I can guarantee the next time you see someone walking or running with a dropped hip on one side or their thigh bone looking like it is going to cross the midline of their body, you will be thinking about good old Coach Gina. There are exercises to target this muscle, but this blog post was more about explaining in greater detail why I love the StairMaster as a supplement to running and if done at 70-80% maximal heart rate, run miles can be substituted for time spent on the StairMaster. My disclaimer for this post... there are other issues that can develop from weak hip musculature! Fight ON! Coach Gina References Dierks, T. A., Manal, K. T., Hamill, J., & Davis, I. S. (2008). Proximal and distal influences on hip and knee kinematics in runners with patellofemoral pain during a prolonged run. Journal of Orthopaedic & Sports Physical Therapy, 39(8), 448-456. Fairclough, J., Hayashi, K., Toumi, H., Lyons, K., Bydder, G., Phillips, N.,…Benjamin, M. (2007). Is iliotibial band syndrome really a friction syndrome? Journal of Science and Medicine in Sport, 10, 74-76. |
Archives
October 2021
Categories |
 RSS Feed
RSS Feed