 Have you ever heard a runner say, “I have runners knee”? Patellofemoral pain syndrome (PFPS), also known as “runners knee” is the most commonly reported running injury and pain is located under the knee or on the inner side of the knee. It is likely related to poor mechanics such as increased hip adduction (thigh bone moving inward towards the center of the body) and hip internal rotation creating malalignment of the lower extremity joints (Noehren et al., 2010). Have you ever seen pictures of yourself, or your friends, running and it looks like the runner is knock-kneed or very little space between the knee of the leg that is in contact with the ground and the leg that is in swing? Hello weak hip abductors! Now it is true that some women have what is called a larger Q-angle (thank you, child-bearing hips!), so the way their thigh bone comes out of the pelvis will be more angled if you will. But you have read about weak hip abductors in my previous blog posts. Refresh your memory by reading the gluteus medius and piriformis blogs!
Iliotibial band syndrome (ITBS) accounts for 12% of all running related injuries (Strauss et al., 2011). ITBS is typically characterized as pain on the outer side of the knee. ITBS is quite interesting because most have accepted the theory that ITBS is a friction syndrome or a rubbing between the bottom portion of the iliotibial band and a bony projection on the end of the thigh bone next to the knee. This area of friction is referred to as the impingement zone. Other theories that cause ITBS exist that make sense and are supported in peer-reviewed scientific literature. For example, the iliotibial band is not a lone structure, but is connected to a thickened portion of the lateral fascia lata, a fibrous tissue that wraps around all the musculature composing the thigh (think sausage casing) and anchors into the femur (thigh bone) (Fairclough et al., 2007). At the other end of the iliotibial band, it is attached to the tensor fascia latae (TFL) muscle, which is guess what??? That’s right, another hip abductor and internal rotator! Okay, it aids in hip flexion too. In a study of 24 distance runners with ITBS, Fredericson and colleagues (2000) noted that all legs afflicted with ITBS had strength deficits in both the gluteus medius and the TFL and, more important to my readers, correcting the strength deficits lead to resolution of the problem. In a lecture by physical therapist Dr. Brent Brookbush, he said, “In my clinic, 9 out of 10 cases of ITBS are from a tight/overactive TFL muscle, not from an impingement at the site of pain". So, all those people that try to foam roll their iliotibial band really aren’t doing a darn thing, because the problem is up higher on the hip and should be foam rolling/applying pressure with a therapeutic device on the TFL. These types of strength deficits can be determined by chiropractors and physical therapists through manual muscle testing. Movement screenings that I offer my runners can also be predictive/prehab for the above issues. Just one of many reasons to hire Run With Gina in your quest for the best half/full marathon training and racing experience possible. Fight ON! Coach Gina Runner Image: Rosy Castro References: Fairclough, J., Hayashi, K., Toumi, H., Lyons, K., Bydder, G., Phillips, N.,…Benjamin, M. (2007). Is iliotibial band syndrome really a friction syndrome? Journal of Science and Medicine in Sport, 10, 74-76. Fredericson, M., Cookingham, C.C., Chaudhari, A.M., Dowdell, B. C., Oestreicher, N., & Sahrmann, S.A. (2000). Hip abduction weakness in distance runners with iliotibial band syndrome. Clinical Journal of Sports Medicine, 37(4-5), 437-439. Noehren, J., Scholz, J., & Davis, I. (2010). The effect of real-time gait retraining on hip kinematics, pain, and function in subjects with patellofemoral pain syndrome. British Journal of Sports Medicine, 45, 691-696. Strauss, E., Kim, S., Calcei, J., & Park, D. (2011). Iliotibial band syndrome: Evaluation and management. Journal of American Academy of Orthopaedic Surgeons 19, 728-736.
3 Comments
 Training for distance running events is a time-consuming endeavor and takes the right balance of work, family, and training to be able to achieve running goals or really any goal. Although any male or female can find the right combination of balance, it seems that this is still more of a challenge for working mothers. Back in 2010-11, I was training for the Boston Marathon; putting in more training than ever, for me. At the time, I ran with several females in a running group and many times I heard them say that they did not have time to train enough to achieve their goals due to family responsibilities. Not being in that situation at the time, I had no room to argue against it or make suggestions. When the 2011 Boston Marathon race day came along, I sat on the bus to the starting line next to a woman that told me that she was a school teacher, had three children under 9-years old, lives in upstate New York and had to train through a brutal winter that year, and due to her family responsibilities, she ran in the dark, in cold temperatures while her children were asleep. Ah ha! When there is a will, there is a way and this random woman modeled positive behaviors towards goal achievement. It is true that some people just want to run without goals and that is okay, but for those who desire to achieve goals and be the best runner they can be, this blog post is for you. Some of this may sound like common sense, but after working one-on-one with distance runners, I can say with certainty that many people see black and white in their life with no shades of grey. The magic can happen in the bleak grey areas, if you shed the light on those invaluable opportunities in your day.
In 2013, Archer and colleagues reviewed data from the American Heritage Time Use Study, which revealed a significant decline in physical activity and increase in sedentary behaviors of mothers between 1965-2010. It will come as no surprise that current sedentary behaviors are associated with screen time accessibility; social media, Apple T.V., Amazon Prime, Netflix…sound familiar anyone? It is true for men, women, and children. Also, a big change from 1965 to current times is the number of mothers in the workforce. Mailey and McAuley (2014) state, over 70% of mothers currently work and 50% of them were active prior to motherhood, yet are no longer active to amounts that benefit health. Working mothers suffer from “role overload” as still often the person responsible for domestic responsibilities on top of work responsibilities. Interestingly and paramount to the current blog post, research has determined that working mothers more than likely have the motivation to change physical activity behaviors, but are lacking in self-efficacy and self-regulatory strategies towards physical activity planning, adoption, and maintenance. Yes! My two favorites from my exercise and sports psychology classes: self-efficacy and self-regulation. This, folks, is where we shed light on the grey areas. Self-efficacy is described as perceived capability based on ability. If one believes he/she does not have the ability to fit training into his/her schedule, then it will be impossible. On a more positive note, self-efficacy (or one’s ability) can be fostered by past performance accomplishments, vicarious experiences, social persuasion, and physiological/affective states. Do you remember what it felt like when you were your fittest or fastest? This is the power of past performance accomplishments and the catalyst for physiological/affective states. When you see your friends on social media accomplishing their goals (say, qualifying for the Boston Marathon), can you literally feel their joy? This is the power of vicarious experiences. Do you see your friends enjoying running groups or getting faster with a personal coach and want the same for yourself? This is power of social persuasion. Self-regulation according to Bandura (1988) is setting goals and planning actions to achieve said goals. In a basic sense, this is problem solving. Problem solve all that stands in the way of you and your goals by identifying the barriers to your success. This is where I think mothers have issues. They know what the barriers are but only see black and white – “I can or cannot achieve that”, instead of “how can I achieve that?”. They think “I cannot because I must go to work, shuttle kids here and there, make dinner, do laundry, and on and on” and “I feel guilty for having ‘me’ time”. Like the woman on the bus in Boston, the only time she could run was when her children were sleeping, so that is what she did. Although not the most ideal option, some people run for 30 minutes during their lunch break and throw in another 30 minutes during their kids practice of whatever sort. Do you get stuck in traffic after work? Why not run while the traffic settles down? That extra 20-30 minutes sitting in traffic could have been 2-4 miles of running. Need to rush home to get the kids to practice? Thank goodness for carpool. Friends and family working towards each other’s goals together. Need to get dinner ready? Three cheers for the old crock pot or Sunday night meal prepping! Can’t get up off the couch because the magnetic pull is too strong? Don’t get on it to begin with. Just lace up your running shoes and hit the pavement first. I can almost guarantee that going for an easy training run will energize you before it will zap you of all that you have. The couch, on the other hand, will suck you in and you will become one with it and drain you of what you have left for the day. I must point out again, a lot of this is common sense, but you must ask yourself, “What stands in the way of me and common sense (the highway to my goals)?”. I was once in a class for coaches and trainers and the lecturer asked, “Who do you think is your biggest competition? The coach down the street? The gym across the street?” Nope, the answer was the couch. And if it is not the couch, it is the barstool at happy hour, the driver’s seat of your car in the slow lane during traffic hour, or maybe just giving more of yourself, not sharing responsibilities with other adults. Teamwork makes the dream work! Fight ON! Coach Gina Runner Images: Darryl, Tricia, and Ruby Sol. Danny and Melissa Magalei. Mark, Cristal, Winter, and Frankie Estrada References: Archer, E., Lavie, C. J., McDonald, S. M., Thomas, D. M., Hébert, J. R., Taverno-Ross, S. E.,…Blair, S. N., (2013). Maternal inactivity: 45-year trend in mothers’ use of time. Mayo Clinic Proceedings, 88(12), 1368-1377 Bandura, A. (1988). Self-regulation of motivation and action through goal systems. In V. Hamilton, G. H. Bower, & N. H. Frijida (Eds.), Cognitive perspectives on emotion and motivation (pp.37-62). Norwell, MA: Kluwer Mailey, E. L., & McAuley, E. (2014). Impact of a brief intervention on physical activity and social cognitive determinates among working mothers: A randomized trial. Journal of Behavioral Medicine, 37, 345-355.  Runners commonly have issues with piriformis syndrome, which is a literal pain in the butt, but it is difficult to determine the cause, so we are going to take a peek at functional anatomy and what research has supported in the treatment of piriformis syndrome.
As a very basic description, the piriformis muscle arises from the front portion of the sacrum (tailbone) and attaches to the femur (thigh bone) and its main function is hip external rotation (thigh bone rotating in an outward direction), aids in hip abduction (thigh away from the body), and aids in hip extension. Hip extension is what creates forward propulsion of the body during running. Due to my experiences with runners, I always think of the orientation and relationship of the pirifomis with the gluteal muscles. Dr. Shirley Sahrmann (2002) discusses the synergistic relationship of the piriformis with the gluteus maximus (GM) in hip extension. The GM is the main muscle of hip extension and the piriformis is one of the “helpers” in hip extension. Like all muscles, the piriformis may be subject to pain associated with muscle shortening from overuse as seen in synergistic dominance. Synergistic dominance is what occurs when a prime mover muscle is shut down and the helper muscle picks up all the work, making it too big for your britches, or just too tight and strong. Dr. Sahrmann does mention that the GM is a muscle that is frequently weak and the piriformis work load increases. Pain may also be from weakness of the muscle from lengthening. This pain is a literal pain in the butt and I unfortunately have had an issue with a weak, lengthened piriformis muscle, as diagnosed by a physical therapist (PT) a few years ago. I specifically remember the PT telling me, “Your marathon training is asking your gluteal muscles and pirifromis to do something they’re not strong enough to do.” I was reminded of this when Dr, Sahrmann said that it is a misconception that participating in a sport places adequate demands on musculature to elicit normal performance. In my case, I thought the dynamic nature of running would be enough strengthening of my running muscles to avoid weaknesses. This is a strong case for prehab exercises. I am all for prevention instead intervention, which is the point of many of my blog posts! Tonley and colleagues discuss piriformis syndrome in a 2010 case report of a subject complaining of “deep buttock pain”. The authors theorized that when the GM is weak, it accommodates abnormal movement patterns at the hip and consequently contributing to excessive lengthening of the pirifomis during functional activities. Muscle testing revealed weakness in the hip abductors, extensors, and external rotators. The subject participated in eight physical therapy sessions during a 3-month intervention. The intervention included exercises that were done at home in three, 4-week progressive exercises phases. Two weeks post intervention the subject declared no buttock pain and increased strength in the hip abductors, extensors, and external rotators. One year post intervention the subject still reported remaining pain free in the buttocks and had resumed sporting activities that were sidelined by pain. I think it is important to point out that synergistic dominance and muscle lengthening is often due to what we are doing when we aren’t running; sitting in the car, sitting at your work space, sitting on the couch, sitting in the bar, sitting with your legs crossed…sitting! Don’t ever forget movement is medicine and the one hour you may spend running, has nothing on all the hours of sitting throughout the day! By the way, if you want to know what the exercises in the pirifomis syndrome case study were, contact me at runwithgina@gmail.com Fight ON! Coach Gina Runner Image: Kay Kay Weir References: Sahrmann, S. A., (2002). Diagnosis and treatment of movement impairment syndromes. Philadelphia, PA: Mosby. Tonley, J. C., Yun, S. M., Kochevar, R. J., Dye, J. A., Farrokhi, S., & Powers, C. M. (2010). Treatment of an individual with piriformis syndrome focusing on hip muscle strengthening and movement reeducation: A case report. Journal of Orthopaedic & Sports Physical Therapy, 40(2), 103-111.  Twice last week I had runners comment to me about the mental aspect of long training runs and endurance races. This is something that many struggle with. It is true there are many factors that play into both the mental and physical “wall,” such as training status, hydration, nutritional practices, and pacing strategies. Regardless of the struggle and failure to meet time goals in a negative mental state, I often hear “but I didn’t give up, I kept going”. There is no doubt that endurance athletes are a special breed of humans. Research using validated psychological instruments has determined that marathon runners have innate, desirable personality profiles of less depression and anxiety and greater emotional stability and psychic vigor compared to non-runners (Raglin, 2001).
None the less, some still have mental demons that try to take them down. As runners, we just want to run, run, and run. However, for those of you that struggle with the demons or those that are ready to find out where there maximal potential as a distance runner is, you should incorporate mental training into your preparation. Mental training can help you prepare to combat the stinking thinking that comes with fatigue, boredom, pain, performance anxiety, and that little devil that takes a spot on your shoulder, negative self-talk. Thanks to some cognitive-behavioral strategies from the sports psychology world, we will be taking a glimpse at some psychological skills training techniques that you can incorporate into training to make you more mentally resilient. Imagery: Imagery is the most researched psychological skill for athletic performance enhancement. Vealy and Greenleaf (2010) discuss the power of imagery in performance enhancement with the simple definition of creating or re-creating a situation or experience in the mind. The most powerful aspect of said practice is how the brain processes virtual images as true stimulus. One way to practice imagery during mental training is to recall positive and negative times in a previous race situation. With the negative image, one practices visualizing overcoming fatigue at that point in the race, turning it into a positive experience for better race outcomes. We all have heard the saying, “seeing is believing”. If you see it in your head, you can help it come to fruition. Play out in your head how you want the race to go and how you want to feel in the moment. With positive images, recall the happiness, strength, and pride you felt and recreate it over and over in your head. Positive self-talk: Self-talk is deployed to reconstruct negative words into positive phrases. Turing self-talk such as “my legs are heavy and hurt” into phrases like “this is a challenge, but I am in it to win it in my head and I have prepared for this day” is an example of positive reconstruction. Positive reconstruction aids in refocusing on the task at hand, therefore augmenting control over running and being able to focus on performance cues, such as reminding yourself, “head up, shoulders relaxed, drive the knees forward, and push off the ground” (Barwood et al., 2008). Goal-setting: Goal-setting is so incredibly vital to marathon running performance and is worthy of its very own future blog post, so I will only give a brief description. Outcome goals are end goals, such as finishing time goals or age group placement goals. These goals, when matched with your level of ability, can help drive training so that you end up at the starting line feeling like a well-oiled machine, thus increasing confidence. Process goals are goals that you turn to throughout the race to help you get through it. An example would be planning when you will take in hydration and nutrition during the race to make sure that your engine remains optimally fueled. Another example is setting goals like “if I feel the need to walk, I will only walk the hydration stations”. A process goal can also be “my only goal is to not walk, because this could take several minutes off my previous marathon effort when I did walk”. Process goals are focusing on finishing the race by breaking it into phases. Some people can handle it my counting miles, whereas others cannot. You can also just count the “kills”, the number of people you pass on the race route that you had been hunting down as your process goal to pass more people than pass you. In a research experiment of psychological skills training, 18 male endurance runners ran for 90 minutes on a treadmill in a room set at 86 degrees Fahrenheit. The runners were blinded to the run pace and distance, but had control of slowing or speeding up the treadmill. Previous research on running in the heat has identified negative mental aspects such as; decreasing motivation, altering arousal, and creating negative mood states. Over the next four days, the runners were then given four, one hour sessions of psychological skills training, including mental imagery, positive self-talk, and goal-setting toward running in the heat. In a subsequent blinded 90 minute treadmill test with the ability to slow or speed the treadmill, the runners ran 8% longer in the same thermal conditions after psychological skills training (Barwood et al., 2008). If the mental aspect of training and racing is something you struggle with, you can find books on Amazon with the skills that I highlighted in this blog post. You must be realistic and know that if you haven’t trained or fueled properly for the distance or are training and racing through a true injury, psychological skills won’t pull you through to a personal best. Fight ON! Coach Gina Runner Image: Kimberly Grady References: Barwood, M. J., Thelwell, R. C., & Tipton, M. J. (2008). Psychological skills training improves exercise performance in the heat. Medicine & Science in Sports & Exercise, 40(2), 387-396. doi: 10.1249/mss.0b013e31815adf31. Raglin, J. S. (2001). Psychological factors in sport performance: The mental health model revisited. Sports Medicine, 31, 875-890. Vealy, R. S., & Greenleaf, C. A. (2010). Seeing is believing: Understanding and using imagery in sports. In J.M. Williams (Ed.), Applied sports psychology: Personal growth to peak performance (6th ed.) (pp. 267-299). New York, NY: McGraw-Hill. 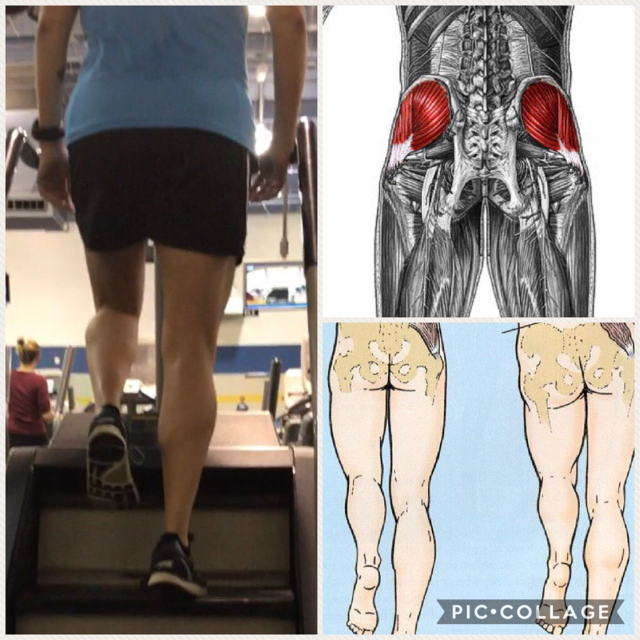 As stated in my previous blog post, “Cross-training can improve run performance”, I absolutely love the StairMaster Gauntlet machine, which is also called the Step Mill (if you didn’t read the post before this one, please do). I decided to expand on why that particular machine is useful for runners that are injured, injury prone, in the off-season, and really any gym goer that wants to move better in their activities of daily living, including just walking down the sidewalk.
In the pic collage above, the picture on the left is me on the StairMaster. Please ignore the scoliosis and slightly turned out stance foot. Haha! Just pointing it out if there are any observant critics out there. The illustration on the top right shows the anatomical location of the gluteus medius (glute med) muscle. The left half of the bottom right illustration demonstrates if the glute med is properly contracting, it will hold the hip opposite of the stance leg level. If it is weak, not contracting, or not “firing” properly, it will cause the opposite hip to drop as shown in the right half of the illustration. As observed in the picture of me, my left hip is being held pretty level with the hip of the stance leg or the leg that is still in contact with the revolving stairs. When we walk or run in the forward direction, we are doing so in the sagittal plane of motion. Glute med stabilizes the hips in the frontal plane of motion, so for simplicity reasons, think left to right or lateral to the body. Given that description, the primary function of glute med is to abduct the hip joint, which means to move lateral, away from the body. A side stepping motion, would be targeting the glut med. This motion, side stepping can be done on the StairMaster. Another reason why I love the machine! Because the glute med has anterior (front), middle, and posterior (rear) fibers it is a contributor to other motions at the hips as well, including hip flexion and extension. Some runners do a dynamic warm-up, mobility exercise, or neuromuscular control exercise called, walking high knees. Basically, walking high knees is an exaggerated hip flexion exercise, where you thrust your knee forward so that your thigh is parallel or just above parallel to the floor. This exercise can be done on the StairMaster. Because the stairs are moving it will provide a greater challenge to the core muscles to stabilize the single leg stance for more bang for your training buck! Additionally, one can do an exaggerated hip extension at toe off of the stance leg while on the StairMaster. I did say that the glut med “contributed” to hip flexion and extension, so there are other prime mover muscles also being targeted, but the point is that the StairMaster has a lot to offer runners and anyone that has weak hip musculature. The above may sound like jibber-jabber, but if I said the words iliotibial band syndrome (ITBS) or patellofemoral pain syndrome (PFSP), suddenly I may be speaking runners language. PFPS, also known as “runner’s knee” accounts for approximately 20% of running related injuries. PFPS occurs when the abductor musculature is weak, allowing for an increase in femoral adduction (thigh moving in) in the frontal plane (Dierks et al., 2008). This is the exact motions that glute med prevents when it is strong. Therefore, weak glute med can contribute to PFPS. Fairclough and colleagues (2007) suggest that ITBS is predominately a proximally based dysfunction of weak hip abductors, which decreases the control of thigh moving laterally. Glute med being one of the hip abductor muscles. When I screen my runners I often find weak gluteus medius muscles on most of them. This muscle is so vital to performance not just when running, but walking and moving in general. I can guarantee the next time you see someone walking or running with a dropped hip on one side or their thigh bone looking like it is going to cross the midline of their body, you will be thinking about good old Coach Gina. There are exercises to target this muscle, but this blog post was more about explaining in greater detail why I love the StairMaster as a supplement to running and if done at 70-80% maximal heart rate, run miles can be substituted for time spent on the StairMaster. My disclaimer for this post... there are other issues that can develop from weak hip musculature! Fight ON! Coach Gina References Dierks, T. A., Manal, K. T., Hamill, J., & Davis, I. S. (2008). Proximal and distal influences on hip and knee kinematics in runners with patellofemoral pain during a prolonged run. Journal of Orthopaedic & Sports Physical Therapy, 39(8), 448-456. Fairclough, J., Hayashi, K., Toumi, H., Lyons, K., Bydder, G., Phillips, N.,…Benjamin, M. (2007). Is iliotibial band syndrome really a friction syndrome? Journal of Science and Medicine in Sport, 10, 74-76.  Exercise physiologists and coaches will say to get better at running, one must run. This is called the specificity of training. To see improvements in run performance, runners must train according to the task by increasing weekly mileage (Loy et al., 1993). Traditional marathon training plans for recreational runners last approximately 18-25 weeks and consist of 4 to 6 days of running up to 25-50 miles or 40-80 km per week (Chorley et al., 2002). Consistent endurance training in higher mileage running facilitates physiological adaptions that allow for a sustained submaximal work effort for a longer period of time (Gibala et al., 2006). Unfortunately, higher weekly mileage places a runner at risk for injury. According to Van Middelkoop and associates (2008), running injury rates increase with weekly running distances beyond 32 km/week. This is only 19 miles a week of running! Okay, who has trained for a marathon and ran much more than 19 miles a week in training? I am going to assume most people, especially as the long run distance ramps up, not to mention many (not all) training programs run up to 20-22 miles as a long run. Never mind the weekly mileage to support that long run. The problem is that some people are injury prone to begin with, regardless if their body has been loaded with the appropriate training distances at appropriates time by a knowledgeable coach. The bottom line is that some people cannot take the ground reaction force, the pounding of the pavement sustained in endurance running. With that being said, alternative training may be the way to go for some.
If you are recovering from an injury or want to substitute some run miles with cross training that can actually benefit your run performance, this is the blog post for you! Runners tend to go to swimming and cycling to substitute their run training, but if it is not done at a great enough intensity, it cannot work as a substitute for run mileage but a supplement. Substitute meaning instead of running and supplement meaning in addition to running to maintain current fitness. When injured, some runners go to water running, which has been shown time and time again to allow runners to maintain their cardiorespiratory fitness achieved through their run training. This allows you to continue training with 85% less force to the body, but the viscosity of the water creates resistance, to make you still “work”. But come on, it is super boring! So let’s take a moment to look at some research to see what else you can do to substitute running miles to improve run performance variables while decreasing run mileage volume. I personally love the StairMaster Gauntlet machine most gyms have. I’m not going to lie, the number one reason why I love it is because it gives you a bird’s eye view of the gym room floor and produces optimal people watching. In a 9-week study conducted by Loy et al. (1993), study participants endurance trained on the StairMaster Gauntlet, four times per week for 30-45 minutes at 70-80% maximal heart rate. At the end of the 9-week training, the participants ran a 1.5 mile time trial and researchers observed a 12% increase in Vo2max and an 8% faster finishing time compared to a 1.5 mile time trial conducted at the beginning of the study. So let me crunch some numbers for demonstration purposes. If someone ran 1.5 mile time trial at a 7:00 min/mi pace, they would have good chances of improving their pace to a 6:27 min/mi pace after 9-weeks of climbing the StairMaster for 30-45 minutes, four times per week at 70-80% maximal heart rate. That is pretty good considering none of these subjects ran. Now this study was in fact conducted on non-runners, but I think it is a strong argument that, some run miles can be substituted for StairMaster Gauntlet climbing in injury prone runners to eliminate the ground reaction force, yet at least maintain cardiorespiratory fitness. Also, as a side note, I personally ran my fastest marathon without speed work, but did 40 minutes on the StairMaster Gauntlet, 2-3 times a week. This folks was long before I studied running, performance, or knew anything remotely close to what I know now. Just because it worked for me, doesn’t mean it will work for everyone. Consider that my disclaimer. A lot of published research on “endurance athletes” is conducted in cycling, instead of running studies. Research by Silder and colleagues (2011) has demonstrated that lower extremity musculature in run/cycle are the same and strength gains in one discipline will transfer to the other. As previously mentioned, many runners substitute running for cycling, but intensity of the activity will determine gains in cardiorespiratory fitness, impacting performance variables. In a 2-week study by Gibala and associates (2006), researchers found that cycling for 30 seconds at maximal intensity for two days with four repetitions, two days with five repetitions, and two days with six repetitions, with four minutes of recovery between reps improved the subjects 30 km time trial by 10%, compared to a 7% improvement in a group of cyclists that cycled at 65% Vo2peak for 90, 105, and 120 minutes for two training days at each time interval. That may not seem like a huge difference, but the most astonishing take-away from this study is that the sprint cyclists total training time over the two week study was 18-27 minutes, including recovery time, whereas the total training time for the endurance cycling group was 630 minutes! I have employed this time saving tactic in some of my run training programs with great success. Again, just because it has worked for some, does not mean it will work for all. Consider that another disclaimer. This blog post does not imply that using the Stairmaster Gauntlet and sprint cycling is all you need to do train for a marathon. Instead it offers alternatives to substituting some run miles in the injury prone runner or cardiorespiratory maintenance in the off season. Nor does this blog post imply that there aren’t other cross-training activities to supplement and/or substitute run training. Lots of research exists to also support maximal strength training and plyometrics to improve run times. Both yoga and Pilates have a place in marathon training as well as a supplement. All possible subjects for future blog posts of course. Fight ON! Coach Gina Runner Image: Ricky Roane, Ultra Runner References Chorley, J. N., Cianca, J. C., Divine, J. G., & Hew, T. D. (2002). Baseline injury risk factors for runners starting a marathon training program. Clinical Journal of Sport Medicine, 12, 18-23. Gibala, M. J., Little, J. P., van Essen, M., Wilkin, G. P., Burgomaster, K. A., Safadar, A., … Tarnopolsky, M. A. (2006). Short-term sprint interval versus traditional endurance training: Similar initial adaptions in human skeletal muscle and exercise performance. Journal of Physiology, 575(Pt 3), 901-911. Loy, S. F., Holland, G. J., Mutton, D. L., Snow, J., Vincent, W. J., Hoffman, J. J., & Shaw, S. (1993). Effects of stair-climbing vs run training on treadmill and track running performance. Medicine and Science in Sports and Exercise, 25(11), 1275-1278. Slider, A., Gleason, K., & Thelen, D. G. (2011). Influence of bicycle seat tube angle and hand position on lower extremity kinematics and neuromuscular control: Implications for triathalon running performance. Journal of Applied Biomechanics, 27, 297-305. Van Middelkoop, M., Kolkman, J., van Ochten, J., Bierma-Zeinstra, S. M. A., & Koes (2008). Risk factors for lower extremity injuries among male marathon runners. Scandinavian Journal of Medicine & Science in Sports, 18, 69  As a recreational marathon runner I am frequently asked by non-runners, “How are your knees holding up? Aren’t you afraid you will get arthritis in your knee and need a knee replacement from running marathons?” It is undeniable that running related injuries are high, and any other disease or dysfunction at up to 79% within a community would be considered epidemic proportions. The injury rates are scary to me, but what is absolutely maddening to me, is people frequently throwing around the arthritis word as if every and only runners would be afflicted with it. In this blog post I will define “arthritis” and I will offer a glimpse of what the research says about what populations are at greatest risk.
More than 100 rheumatic diseases exist, but the two most common types are rheumatoid arthritis (RA) and osteoarthritis (OA), often times just referred to as arthritis. Although the etiology, risk factors, and prevalence of RA and OA are different, they are both characterized by pain in the joints and debilitating functional limitations (Stone & Baker, 2014). The largest difference in RA and OA is in their physiological mechanisms. The exact cause of RA is unknown and is considered an autoimmune disease which is possibly the result of an interaction between genetic disposition, environmental factors, and chance. RA is a systemic inflammatory disease linked to cardiovascular, pulmonary, and gastrointestinal diseases, in addiction to cancer and is sadly observed more in females (Gibofsky, 2014). The good news is, US studies have noted a progressive decline in RA prevalence since the early 1960s (Helmick et al., 2008). Osteoarthritis (OA) is distinguished by degeneration of the articular cartilage, progressing to eventual cartilage loss, creating a bone on bone scenario of weight bearing joints, most commonly the knee and hip. OA is the leading cause of knee and hip joint replacement (Rooney, 2004). The cause of OA is multifactorial with the largest contributing factors including, higher body mass index (BMI), previous traumatic knee injury, occupational activity, and increased age (Richmond et al., 2013). I don’t know about you, but I did not see being a runner as one of the largest risk factors associated with OA or joint replacement. Unlike the prevalence of RA decreasing, previous research showed OA increased 22% from 1995-2008 (Lawrence et al., 2008) and continues to rise. If you have read the “about” section on my website, you know that I work as a registered dental hygienist and I have done so for 19 years. One of the first things I do at the beginning of my patients appointment is to go over their medical history. I treat several patients a week that have had a joint replacement. I can say with certainty that I have never had a patient acquire arthritis or need a joint replacement from marathon running. I think we all are aware of the prevalence of overweight and obesity in our society. Does anyone think that the increase in osteoarthritis may be parallel with the overweight and obesity epidemic? Does anyone think that the increase in osteoarthritis may be parallel with the longer life expectancy due to medical interventions? Does anyone think that there are more traumatic youth knee injuries from early sports specialization more common in the last couple of decades? OA is actually highest in former female soccer players with a previous anterior cruciate ligament (ACL) injury and football players that take traumatic hits and are often times obese. You see large football players and although they may be athletes, I see a Ford 250 Extended Cab truck, rolling around on Honda Civic tires. Imagine it, those tires are going to breakdown sooner than later. Runners can be at risk for OA if they constantly run through injury without proper treatment and time off, which cumulatively can lend itself to the previous injury risk factor. A runner and their coach if they have one, need to be mindful of the laws of biomechanics I wrote about in my injury epidemic blog post. If you haven't read that blog post, please do. A runner can also be at risk if they have poor mechanics with muscular imbalances. This would be similar to a car having it’s alignment off and the tires wear unevenly. The same thing can happen with the meniscus of the knee. However, these risk factors are extremely low for developing arthritis in the knee if not coupled with higher BMI, previous knee injury, occupational activity, and/or increased age. To say that runners will ruin their knees, get arthritis, or need a joint replacement because of running is a fallacy. Fight ON, Coach Gina Runner Image: Ara Miralles References: Gibofsky, A. (2014). Epidemiology, pathophysiology, and diagnosis of rheumatoid arthritis: synopsis. American Journal of Managed Care, S128-S135. Helmick, C. G., Felson, D. T., Lawrence, R. C., Gabriel, S., Hirsch, R., Kwoh, C. K….Stone, J. H. (2008). Estimates of the prevalence of arthritis and other rheumatic conditions in the United States: Part I. Arthritis & Rheumatism, 58(1), 15-25. Richmond, S. A., Fukuchi, R. K., Ezzat, A., Schneider, K., Schneider, G., & Emery, C. A. (2013). Are joint injury, sport activity, physical activity, obesity, or occupational activities predictors for osteoarthritis? A systematic review. Journal of Orthopaedic & Sports Physical Therapy, 43(8), 515-524. Rooney, J. (2004). Don’t get out: Understanding the difference between osteoarthritis andrheumatoid arthritis. Nursing Made Incredibly Easy, 2(2), 26-35. Stone, R. C., & Baker, J. (2014). ) Physical activity, age, and arthritis: Exploring the relationships of major risk factors on biopsychosocial symptomology and disease status. Journal of Aging and Physical Activity, 22, 314-323.  Yesterday I spent the morning cheering on runners at the inaugural San Diego Beach and Bay Half Marathon. It was a great time and I reached a personal record! That’s right, I reached a personal record in receiving the most sweaty hugs in one day. I could have wrung some of those runners out and had buckets of sweat. Sweating is good though, it helps thermal regulate the body. What is your body losing in that sweat and how should you replace it to help regulate body temperature and metabolic processes? All those sweaty hugs inspired this blog!
Over the years, the recommendations for hydrating during endurance exercise have changed. The first recommendation was to drink, “as much as tolerable”. Dr. Timothy Noakes stated in 2003 that there were 250 documented cases of hyponatremia (low blood sodium) from 1985-2001, with the runners reporting that they had followed the standard recommendation of “drink as much as tolerable”. One is at risk for hyponatremia not only when they sweat and don’t replace it with fluids, but when they sweat and they rehydrate with lots of water only, basically diluting the sodium in their blood. Our bodies are actually made up of 60% water and rehydrating with water is fine if you are running for less than an hour, but when running for more than an hour your fluids should also be supplemented with a sports drink containing electrolytes. Sweating isn’t just about losing fluid. It isn’t water out, water in, to maintain balance. Von Duvillard and colleagues (2008) refer to fluid balance as a complex process and exercise challenges the body to regulate fluid and electrolytes. The electrolytes, sodium and potassium are important micronutrients for maintaining optimal performance in half and full marathon running. Sodium and potassium replacement are important in endurance exercise not just for hydration maintenance, but for maintaining plasma volume. Sodium maintains or increases plasma volume by improving water and glucose (sugar) absorption in the small intestine, therefore aiding performance variables. Benardot (2012) refers to performance variables as the ability to maintain sweat rate, deliver nutrients to cells, and clear metabolic waste from cells. Yikes! The body is a machine and just like your car, you have to keep it fueled (or charged these days), lubricated, filters in check, tires pumped up, and alignment correct. Later, Noakes suggested that runners should drink ad libitum, which is as needed, dictated by thirst. However, some will say that if you wait until you are thirsty, then dehydration has already set in. Drink too little, end up in the medical tent dehydrated! Drink too much water and end up in the medical tent with hyponatremia! Drink too much Gatorade on the course, along with salt tablets, and sodium containing nutrition, end up in the medical tent with hypernatremia (high blood sodium)! So what is the recommended formula? According to the American College of Sports Medicine (ACSM) the current recommendation to best maintain fluid balance and optimal performance variables is drinking 3-8 ounces of water every 15-20 minutes for exercise less than 60 minutes and 3-8 ounces of sports drink every 15-20 minutes for exercise over 60 minutes. This is a pretty large spread and variables that should be considered are metabolic requirements, climate, altitude, duration, clothing, and individual sweat rates (Sawka et al., 2007). I personally have high hydration needs. I ran eight miles at an aerobic pace and drank 20 ounces of fluids, which was close to 5 ounces for every 16 minutes. This was conservative for my needs, taking the length of the run into consideration. Had I run longer, I would have needed to drink more fluids earlier on to better maintain my hydration status. The key is to play around with your fluids during your long training runs. Keep a log of how much you drank and how you felt during the run and equally important, how you felt the remainder of the day. Okay, so the next blog will be about arthritis! Fight ON! Coach Gina References Benardot, D. (2012). Advanced sports nutrition (2nd ed). Champaign, IL: Human Kinetics. Noakes, T. (2003). Fluid replacement during marathon running. Clinical Journal of SPORT MEDICINE, 13(5), 309-318. Sawaka, M. N., Burke, L. M., Eichner, E. R., Maughan, R. J., Montain, S. J., & Stachenfeld, N. S. (2007). Exercise and fluid replacement. Medicine & Science in Sports & Exercise, 39(2), 377-390. Von Duillard, S.P., Arciero, P. J., Tietjen-Smith, T., & Alford, K. (2008). Sports drinks, exercise training, and competition. Current Sports Medicine Reports, 7(4), 202-208.  Since the running boom began 40 + years ago, participation in marathon running events has risen from under 30,000 people per year to 507,000 participants per year (1). How often have you or somebody you know, signed up for a running event and became injured before race day? As marathon participation has risen, so has running related injuries. Sadly, the scientific literature on running injuries notes injury rates somewhere between 19-79% annually. The spread is huge, however much of the literature considers time off from running due to pain as an injury, even when nonspecific in origin. None the less, even at the minimum of 19%, this is far too great. Unfortunately, I have witnessed many times people running despite an injury. Quite honestly, I am not a fan of seeing runners wearing bracing devices. More than likely, if there isn’t an organic structural issue going on, whatever the runner is trying to band aid up could have been prevented or treated with proper run training, chiropractic, massage, gait training, and the assistance of corrective exercises. Bracing and taping often times helps symptoms in the short term, but doesn’t treat the dysfunction and will only initiate a cascade of training setbacks, creating barriers to improvement and goal achievement.
In addition to improper run training loading, too great intensity of running, and too little rest/recovery, many injuries are due to poor biomechanics, such as hip internal rotation, hip adduction (the thigh bone moving towards the midline of the body), and contralateral pelvic drop (pelvic drop of the non-weight bearing leg). Although pain exists in one part of the body, the problem can actually be from a more distant site. I like to imagine muscle imbalances as muscles playing tug of war and the bone is actually the rope. The body will take the path of least resistance, which means that the tighter, overactive muscle will pull the bone in one direction and the weaker opposing muscle will allow for excessive, inefficient movements. This causes improper distribution of the ground reaction force up the kinetic chain or joint segments of the body. Safe and efficient running requires an optimal orchestration of many muscles and joint movements and their movements are referred to as internal factors related to each individual runner. Part of understanding injury, is understanding how the body responds to forces placed on it. In the study of biomechanics I was introduced to Wolff’s and Davis’ law, which respectively state that bone and soft tissues remodel along the lines of stress. When we typically hear or read the word “remodel” we think of something nice or better. If stress or the load is undertaken in a biomechanically correct form, then the stress will be positive and it will strengthen tissues and bone. However, with poor movements, the lines of stress will be deviated from the intended path and can breakdown tissues and bone, which would in fact be a remodel from its former or intended state, leading to dysfunction. Running with a biomechanically correct stride has positive effects on bone. Bone mineral density (BMD), a measure of bone mass is greater in exercised limbs as a consequence of Wolff’s law, compared to sedentary individuals (2) and females have shown an increase of 0.9% BMD per year in exercised limbs at the loading site of impact (3). I will admit, I am a bit of a nerd, but knowing this stuff is what helps me correct training errors of my runners and to help keep me out of fracture city like I experienced when I first took up distance running. As mentioned, running is actually good for bone, but not so much if your stabilizer muscles aren’t in good working order to do just that. There are three planes of motion that our bodies move in and running occurs in one, the sagittal plane. I think that an error many runners make is that they neglect some of the other muscles that help support running through stabilizing in the other two planes of motion. Only training the muscles that work in one plane is sort of like the shirtless guy you see running in a 5k with the well-defined chest muscles from his 100 push-ups a day, but as you see him from behind, his back is giggling, without definition. I have seen this friends and it is the oddest thing. Structurally this can create issues. Most people have heard of the piriformis and gluteus medius muscles. These are muscles that runners commonly have issues with and guess what? They primarily move in the other planes of motions, although the piriformis also aids in hip extension in the sagittal plane. The reasons noted above for contributing to running injuries is not at all a complete list of potential internal and external factors that contribute to injury. However, knowing this information is a great aid in decreasing injury possibilities and building more efficient runners. My runners that are local in San Diego County, receive a screening before starting a marathon training program with me and have proven to be informative and valuable. I can also screen runners that train with other coaches and use other training plans. So don’t be shy to contact me to use my services. In a blog next week, I am looking forward to giving you the appropriate answer to the question I’m sure every runner has been asked before, ”aren’t you afraid you will get arthritis from running?” Please feel free to message me with questions. Fight ON! Coach Gina Runner Image: Christian Pratt References: 1. Fields, K. B., (2011). Running injuries: Changing trends and demographics. Current Sports Medicine Reports, 10(5), 299-303. doi: 10.1249/JSR.0b013e31822d403f. 2. Harrast, M. A., & Colonno, D. (2010). Stress fractures in runners. Clinics in Sports Medicine, 29(3): 399-416. doi: 10.1016/j.csm.2010.03.001. 3. Nevill, A. M., Burrows, M., Holder, R. L., Bird, S., & Simpson, D. Does lower-body BMD develop at the expense of upper-body BMD in female runners? Medicine and Science in Sports and Exercise, 35(10), 1733-1739.  I received an email from a runner today and upon reading it, I thought, “well this is something that is blog-worthy”. Here is a message to me from an anonymous runner:
“I have to confess coach: I have not been following the schedule. We have had long days with early starts, rain, too much beer and not much sleep. I've managed to put in a few miles.” What I love most about this message is not that she is being honest with me, but that she is being honest with herself. As recreational half and full marathon runners, we typically have a lot on our plate; work, family, volunteer, and run training responsibilities. If we want to do it all, we need to learn to balance it all. The runner quoted above doesn’t have a time goal for her race and she is happy with doing what she can do with the time that she can commit to training. I get runners that are aiming to run a personal best, qualify for the Boston Marathon, and runners like my example runner. Any type of runner is cool with me, as long as each individual is honest with him/herself, including understanding their inherent ability as a runner. You can train to your ceiling, your natural level of ability, but what that is for me and what that is for runner A, B, C….is different and more importantly, the process to find out what that is takes time and requires both patience and persistence. In addition to run training, nutrition, health and fitness, future blogs will cover really important topics that help runners achieve their goals, such as realistic goal-setting, ways to foster self-efficacy, which is confidence in your ability to achieve intended results, and learning how to identify one’s barriers to success. Lots of great information coming in the following weeks, months, and hopefully years, so keep checking the website regularly! Next up, we will be taking a look at injuries in our distant running community. Until then, happy running and feel free to email me if there are any topics you wish to be covered in the future or need some immediate questions answered. Fight ON, Coach Gina Runner Image: Art Santos |
Archives
October 2021
Categories |
 RSS Feed
RSS Feed